
We’ve all had those patients… and indeed those moments.
The one where the client is looking intently over your shoulder and putting you off your game. Or maybe you’re working with a severely compromised patient whose blood pressure has bottomed out. Or maybe this patient has already had a million IV’s placed in the preceding days and there’s just not much left to work with.
Whatever the reason, sometimes getting IV access for euthanasia is just not as easy as we would like it to be. As a vet team who deliver care to our patients at home, we’re often faced with less than ideal conditions for placing IV’s. There’s no ‘out the back’ to escape to. No well-trained nurse to work their magic on frightened patients. Most likely, we’re stuck half underneath a bed because that’s the patient’s favourite place, or we’re working with a family who needed an evening appointment so the lighting can at best be described as ‘mood lighting’.
Sometimes, it’s neither the patient or environmental factors that throw us. We may simply be faced with a client who is particularly distraught and asking them to release the pet from the bear hug it’s held in, may just be too big of an ask in that crucial moment of grief.
If you’re like me, you may have subconsciously absorbed messages during your early training that there is a right and a wrong way to perform a euthanasia. In essence, IV barbiturate is right… anything else is less than ideal and if you’re reaching for it something has probably gone ‘wrong’.
Since delving into the palliative care world, I have learnt to question myself more, particularly when it comes to any clean-cut definitions of right and wrong. Palliative care is very much about finding the best solution for the patient in front of you and as such, I have developed a new found respect for non-IV routes for delivery of barbiturate.
Why do we go IV in the first place?
We go IV because it delivers our barbiturate to where we need it to go in rapid fashion. Usually we see loss of consciousness and cessation of cardiac output under 2 minutes. This is often what we are aiming for and most of the time IV is going to be my preferred method of delivery. But not always. There are times where patient or client factors present opportunities to choose a better path.
- If you’ve already attempted peripheral IV placement with no success, maybe it’s not appropriate to put the patient, and the client if they’re watching, through the process of another needle stick. Client confidence is a fragile thing. If you haven’t succeeded in placement on your second attempt, never try for a third. Stop, regroup and move confidently to plan B.
- If the patient is anesthetised* and resting comfortably with your cocktail of pre-euthanasia medications, perhaps this client would actually prefer a more gradual passing over a period of time, such as we see with intra-organ injections. For many vets, this is about framing the conversation correctly. Saying something like, ‘once he/she is relaxed and sleeping from the first dose of medication, I’m going to give a second dose via the best route for him/her.’ This allows you flexibility and avoids priming the client for an IV injection alone should your plans change mid-way through the appointment. Think this will take too long for euthanasia appointments in clinic? Time yourself and look at critically at how your structure the flow of your appointment. Time savings can be made in many places without impacting on the client experience or patient care.
- For clients who have been through an intense period of illness with their pet, many will be beginning to experience a level of caregiver fatigue. This is a well recognised concern in human palliative care and I believe managing this in our clients is increasingly part of our duty of care. For these families we can choose to actively spare them the ‘medicalisation’ of the euthanasia process by avoiding the placement of an IV. Let them keep cuddling that pet and deliver your barbiturate IH or IP instead. The way we approach this last appointment and the care we show our clients at this time has a surprising impact on the intensity and duration of their grief, as well as their time to recovery following the passing of the pet1. You have the power to impact this. Use it!
Addressing the failure myth
Too many vets I meet, have deeply seated beliefs that their ability to place an IV catheter or deliver a clean IV stick in a euthanasia situation is a reflection of their skill and ability as a vet. Not only is this mindset likely to prevent you performing at your best, but working with old, unwell, unstable, decompensating patients is going to throw you your fair share of challenges. It’s just the way it is. Your skill as a vet, is much more linked to your ability to think on your feet, know and navigate your alternate options, deliver the best possible welfare outcome for your patient and simultaneously support the wellbeing of the clients who are in your care. It’s a lot to juggle. Let go of the mind game stuff.
Faster is not always better
When a client reaches out to us for euthanasia here at Sunset, we start by asking a lot of questions. One of which is whether they’ve been through a euthanasia before. One of the most common bits of feedback we hear from clients who were unhappy with their previous euthanasia experience is that the pet passed too quickly. This is often more confronting than we realise for clients and they are left feeling like they had no time to process what was happening.
As a profession, we need to remember the gravity of what we are doing in a euthanasia appointment. Our language is often about alleviating suffering and preventing further distress and at times there is definitely a requirement for speed if a patient is in crisis. But it’s important to note that what we are also doing is taking a life. To do this too quickly and with apparent ‘ease’ (for veterinarians who aim to shield their clients much of the process) can be to diminish the client’s ability to experience and fully understand the moment. Let them see your process. Be prepared to remain in the consult room while you sedate or place your IV. Be open, compassionate and transparent about every stage in the process. Don’t rush.
Alternate routes to consider
There are literally dozens of alternative routes to use if your first port of call doesn’t work out or isn’t the best plan for the patient or client. You may try for some alternate veins… medial saphenous, the medial branch of the cephalic on the ventral leg and the dorsal pedal vein being a few favourites from those of us here in the home euthanasia trenches.
For intra-organ injections, learn your landmarks and practice your techniques on cadavers wherever possible to increase your confidence and success rate. Think about how you will approach a patient with ascites or peripheral oedema and think about how this disease state will impact the patient’s physiological state… which route will be most appropriate?
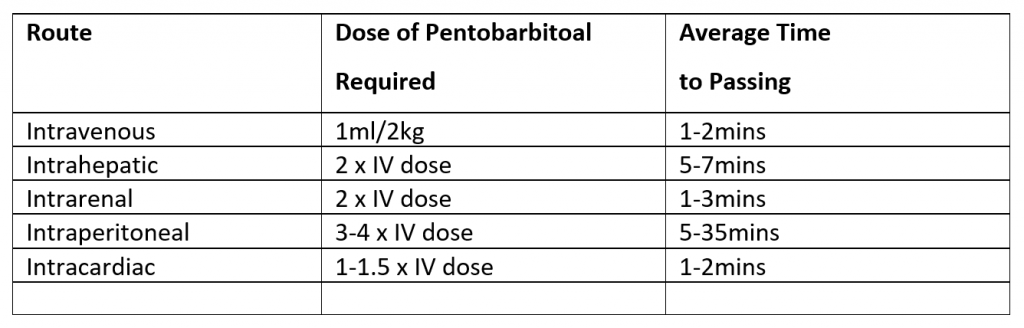
Need a quick cheat sheet to weigh up your options in a hurry, see below, or track down a copy of Dr Kathy Cooney’s Euthanasia Techniques textbook2, available from Wiley Publishers for a more in-depth look.
*At Sunset Vets we advocate for all patients to be at an anaesthesia plane prior to the delivery of barbiturate, including for direct IV injections. Anaesthesia plane is a requirement for all intra-organ injections3. Want to know more about our pre-euth medication protocols, feel free to get in touch.
References
- Herbert R, Prigerson H, Schultz R, et al. Preparing caregivers for the death of a loved one: a theoretical framework and suggestions for future research. Journal of Palliative Medicine. 2006; 9: 1164-9.
- Cooney Ka, Chapell J, Callan RD, Connally BA. Veterinary Euthanasia Techniques: A Practical Guide. Ames, IA: Wiley Blackwell, 2012.
- AVMA Guidelines for Euthanasia of Animals 2013. Available at: https://www.avma.org/KB/Policies/Documents/euthanasia.pdf. Accessed 19th Jan 2019.


